
Two days before he nearly died, Ryan Eisner felt great. In fact, if you’d asked him, he would’ve told you he was in the best shape of his life.
Ryan had grown up playing basketball in Bayside, a neighborhood in the New York City borough of Queens. As a freshman, he made the varsity at Bayside High. Even though he stood only 5 foot 10 inches tall, he had an explosive first step and a nose for the basket. By the end of his junior year, he’d established himself as a prolific scorer, and colleges began to contact him.
That summer, Ryan showcased his talents in a tournament featuring a who’s who of young prospects, including future National Basketball Association players like Joakim Noah and J.R. Smith. In one of those competitions, as a gym full of coaches watched, Ryan scored at will. To him, the basket looked as big as an ocean, and every shot he threw up seemed to splash in. After one quarter, he’d already rung up 20 points.
On the first play of the second period, Ryan got the ball and made a quick juke toward the basket. The fake sent the defender flying into the air, and when he came down, he landed on Ryan’s leg.
When people sever ligaments in their knees, many describe feeling a pop. Or hearing one. But Ryan didn’t feel or hear anything. Still, his anterior cruciate ligament had snapped. And just like that, his high school basketball career ended.
Surgeons repaired the ACL that winter, and Ryan worked hard to rehabilitate his knee. While the big universities no longer showed interest in a short kid with the surgically repaired knee, some smaller schools still saw promise in him. When Drew University, a 1,500-student liberal arts college in New Jersey, offered him the chance to come and play, Ryan took it.
Playing college basketball had been Ryan’s lifelong dream. And even though that dream now had a few asterisks—smaller stage, gimpy knee that couldn’t do what it used to—he made the most of his chance. As a freshman guard, he came off the bench. He showed enough hustle and talent to earn some starts as a sophomore, scoring as many as 14 points in a game. When the season ended, the coach took him aside and said, “Listen, you’re going to have an opportunity next year. This will be your team to drive.”
Ryan worked out hard all summer and showed up for his junior year in 2007 as fit as he’d ever been. “I was really excited. I was ready to go,” he says. “I knew I was going to blow it out of the water.”
At the first practice on a Tuesday morning in August, he registered the lowest body-fat percentage on the team. The coaches had the players run a mile around the track, and, again, Ryan bested all of his teammates. But during a series of sprints that followed, Ryan did something he’d never done during a workout: He vomited.
That afternoon, the players gathered for a second practice at the gym. Ryan plodded through the ball-handling drills and a scrimmage. The session ended with a series of “suicides,” where players sprint up and down the court. Ryan finished the drills, but barely.
When he got back to his dorm, he felt as if someone had sucked the life from his body. He lay down to gather his energy. When he tried to get back up after a few minutes, his head felt heavier than a boulder. Sure, two practices the first day back should leave you tired. But not like this.
Ryan went to the student health service. A nurse took his temperature: 104 degrees. Immediately, the on-call doctor sent him to a nearby hospital. There, a physician in the ER diagnosed him with a respiratory virus. The doctor administered some intravenous fluids and prescribed some steroids to help Ryan’s breathing, then released him.
But the next morning brought no relief. Ryan’s head still felt like it was on fire. When he walked to the bathroom, he grew dizzy, and his legs buckled. He called his parents. “You’ve got to come get me,” he croaked. “I’m really, really sick.” Mitchell and Karen Eisner drove the hour to New Jersey to pick up their son, then whisked him to a doctor they knew. She listened to his heart and his lungs but didn’t hear anything out of the ordinary. “It’s a virus,” the doctor reassured the Eisners. “It will run its course over time.” In the meantime, she told Ryan, “Go home. Get some rest.”
By the next morning, Ryan’s body shook uncontrollably with the chills. His fingers had turned blue. His mother brought him to a different doctor, who took Ryan’s vitals. “He had the heart rate of a guy running a marathon,” remembers Mitchell Eisner. With Ryan’s fever also continuing to burn out of control, the physician sent him straight to the emergency room.
As his mother drove him to the hospital, Ryan huddled in the passenger seat, shivering and laboring with each breath. Occasionally, he’d repeat a single sentence: “Mom, I think I’m going to die.” But at the Long Island Jewish Medical Center-North Shore, all of Ryan’s tests again came back negative. And, once more, the doctors instructed him to go home and rest.
Mitchell Eisner felt like he was caught in a bad dream. Please, he pleaded with the physicians, don’t turn us away. In just two days, his son had gone from fine to dramatically ill. He felt certain that Ryan was suffering from more than a garden-variety virus. “You need to keep him here,” Mitchell told the doctors. “You need to figure out what’s wrong with him.”
There Will Be Blood
Dr. Charles Esmon has devoted pretty much his entire life to studying blood and how it clots. As a graduate student at Washington University in St. Louis, he haunted slaughterhouses, collecting buckets of the red liquid from cows for analysis. When it came time to establish his own independent research laboratory in the mid-1970s, one of the reasons he chose Oklahoma City was its stockyards. “We could get about 100 gallons of blood every two weeks,” he recalls. “And that helped us learn a lot.”
In his lab at the Oklahoma Medical Research Foundation, Esmon figured out how to isolate and purify a particular protein from the bovine blood. That protein, known as protein C, occurs naturally in the blood of cows—and people—to prevent clotting.
At about that same time, a pair of researchers identified a rare condition in children born without protein C. Without the protein, blood coagulated in their veins, a life-threatening condition that manifested itself in the form of enormous purplish blotches on the skin. As he gazed at photos of the infants in a medical journal, Esmon realized that their symptoms looked an awful lot like those of people suffering from another condition: meningococcemia, a potentially fatal bacterial infection.
What, Esmon wondered, would happen if he isolated protein C from human blood? Could he take that protein, chemically activate it, and then use it to save people infected with meningococcemia?
Building on his work with bovine samples, Esmon devised a way to isolate protein C from human blood. In collaboration with fellow OMRF researcher Dr. Fletcher Taylor, Esmon tested his theory in pre-clinical models. Repeatedly, activated protein C showed promise for treating the infection. But the experiments suggested that the compound might rescue not only people with meningococcemia but also those suffering from other life-threatening blood infections, a broad category of illness known as sepsis.
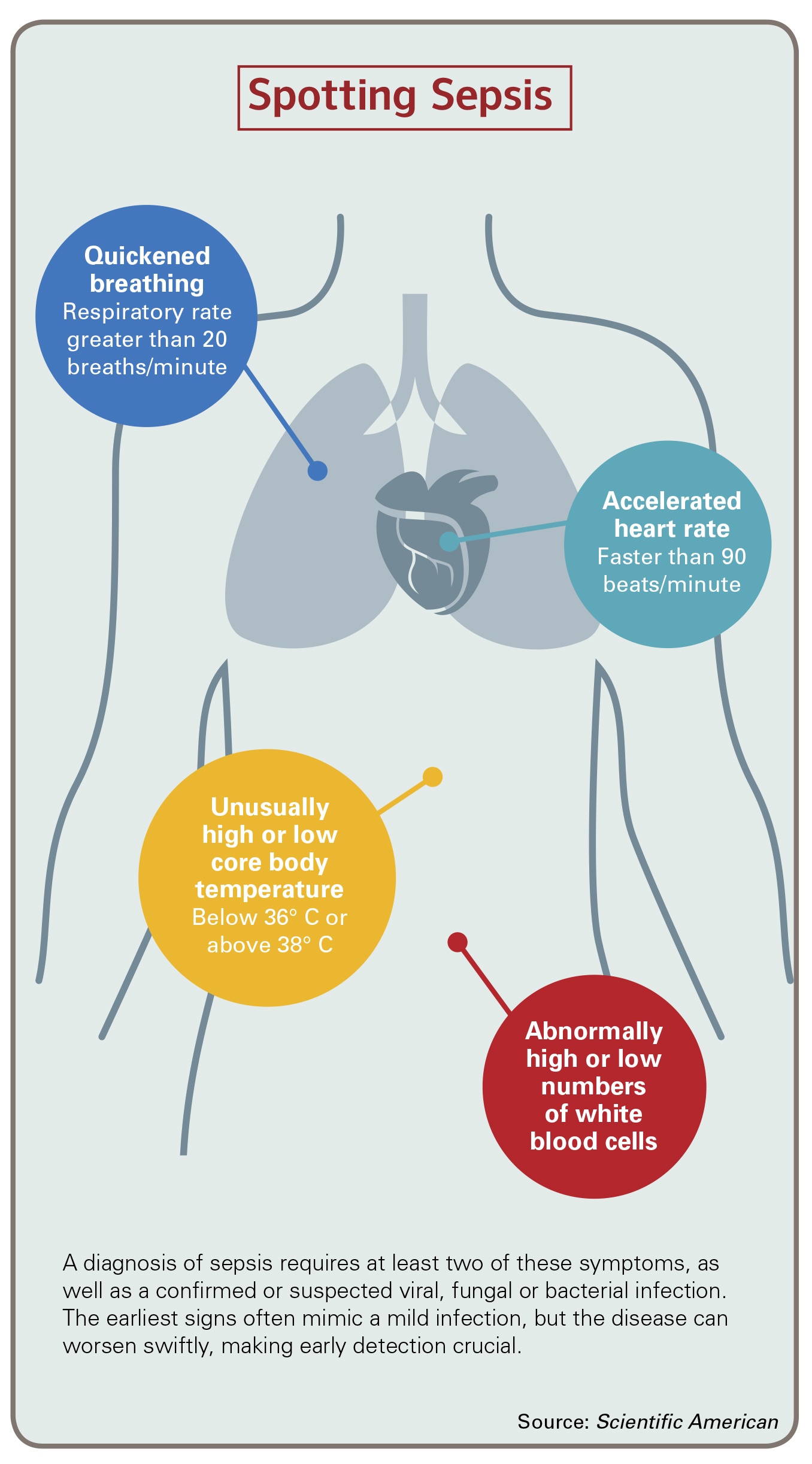
Sepsis can begin in many different ways: a virus, a skin infection, food poisoning, or a traumatic injury like a bullet wound or car crash. But not everyone who experiences these conditions becomes septic. What distinguishes the illness from its more innocuous counterparts is that in sepsis, the body’s immune system fails to repel the unwelcome pathogen (a virus, bacteria or fungus) that has entered the body. When the invader hangs around long enough, it can find its way into the blood stream. And then, says Esmon, “All heck breaks loose.”
The body responds by calling in its heaviest artillery: an overwhelming, system-wide counterattack. Blood vessels become inflamed, and their cell walls leak fluid. The clotting system goes awry, simultaneously causing bleeding and throwing clots that block the tiny blood vessels that feed organs.
Sepsis has proven particularly problematic to treat because of its chameleonic nature, which can render it indistinguishable from other, less dangerous conditions. So physicians often miss its early signs. The frightening speed at which sepsis progresses compounds the problem, moving in a matter of hours from an apparently mild infection to life-threatening shock—a drastic drop in blood pressure, often followed by organ failure. As a result, doctors are often too late to launch the standard courses of treatment, which include antibiotics to wipe out the infection, medications to keep blood pressure from nosediving, and a ventilator to pump oxygen-rich air into patients’ lungs. And the later these treatments start, the worse a patient’s chance of survival.
All told, roughly one-third of the people who develop sepsis die. It’s the leading killer in intensive care units in the US, claiming an estimated 250,000 lives each year. ICU doctors have a saying about the condition: “Fine in the morning, dead in the evening.”
“You’d Better Start Praying”
When Mitchell Eisner refused to take his son home from Long Island Jewish Medical Center-North Shore, physicians at the hospital finally agreed to re-examine Ryan. And when they did, they determined he was suffering from pneumonia.
The doctors admitted him to the hospital and started him on antibiotics. At long last, Ryan had a diagnosis and a course of treatment. “We thought he was going to stay overnight and be fine,” says Karen Eisner. Relieved and exhausted, she headed home for the night to get some rest, while Mitchell stayed. A few hours later, at Ryan’s request, Mitchell drove to the house to pick up some clothing, books and basketball magazines. When he returned to the hospital 45 minutes later, he found five white-coated doctors huddled around his son’s bed.
“Hey, what’s going on?” Mitchell asked.
“He crashed,” said one of the physicians.
“What do you mean, ‘crashed’?”
The physician in charge turned to Mitchell. “He’s very sick. We had to intubate.” A ventilator huffed in the background, pushing oxygen through a tube that now ran out of Ryan’s mouth. “You’d better start praying,” the doctor said. “He’s going to die.”
Mitchell could scarcely process what he’d just heard. Less than an hour ago, he’d been chatting with his 20-year-old son, a college athlete in tip-top shape. And now a doctor was telling him Ryan was as good as dead?
Finally, Mitchell managed to stammer, “When?”
“Anytime,” the doctor answered. “It’s septic shock.”
Shock to the System
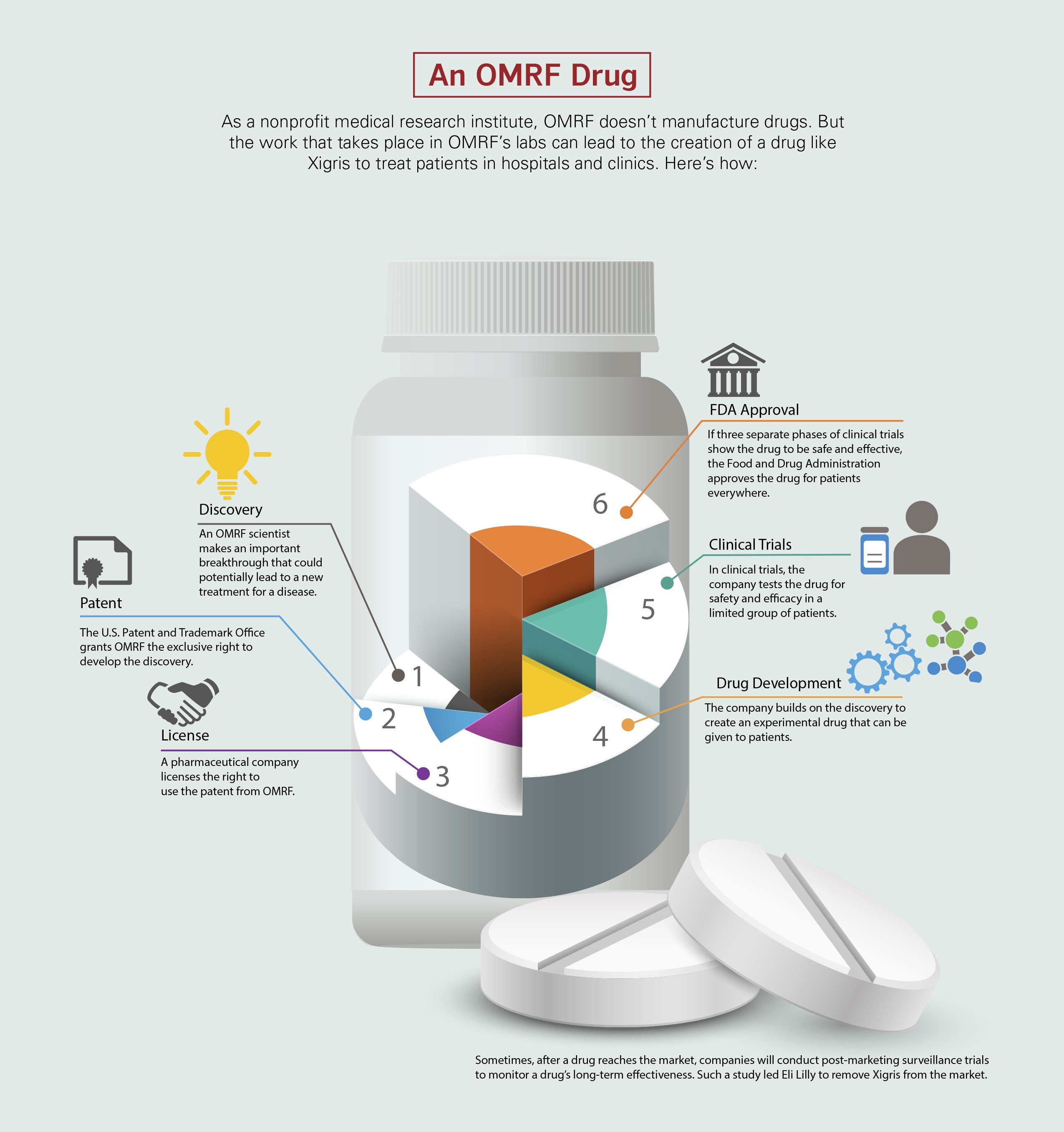
For decades, researchers had been searching for more effective treatments for sepsis. In the 1980s and 1990s, more than 20 experimental drugs failed to show any benefit in treating the condition. But in 2001, the Food and Drug Administration approved Xigris (rhymes with tigress), a synthetic version of the activated protein C Drs. Charles Esmon and Fletcher Taylor had pioneered in their experiments at OMRF. In a clinical trial that had involved 1,700 patients, the drug, which was manufactured by the pharmaceutical giant Eli Lilly and Company, had cut mortality in those with severe sepsis by 24 percent.
The medical community, though, didn’t universally embrace the drug. Half of the panel members who initially reviewed Xigris for the FDA said the agency should not approve the drug without more data. Although the FDA went ahead and gave Xigris the green light, it limited the drug’s use to only the sickest patients. Subsequent trials ordered by the FDA failed to show benefit when doctors administered the drug to less ill adults or to children with severe sepsis.
Xigris was also hampered by a serious side effect, internal bleeding. And its $6,800 price tag (a figure that drew heavy criticism of Eli Lilly) further limited its use.
Still, many critical care specialists felt that Xigris served an important unmet therapeutic need. Dr. Gary Kinasewitz, chief of Pulmonary and Critical Care in the University of Oklahoma Health Science Center’s Department of Internal Medicine, participated in the clinical trial that led to the drug’s approval. Once Xigris reached the market, he and his colleagues at OU Medical Center continued to prescribe the drug regularly. “We probably used Xigris 100 times a year,” he says.
Kinasewitz believes that Xigris helped rescue some of his patients in septic shock. But with doctors simultaneously administering so many different forms of sepsis therapy—multiple antibiotics, fluids, ventilators, blood pressure drugs—it can be virtually impossible to say what, exactly, turned the tide for an individual patient. Still, Kinasewitz remembers one particular case where he feels confident Xigris made the difference between life and death.
He gave the drug to a woman suffering from severe septic shock, and her condition improved dramatically. After 96 hours, the recommended duration of treatment, Kinasewitz stopped the treatment. “Within several hours, her blood pressure had dropped, and she was significantly worse.” Kinasewitz decided to re-start her on Xigris, and the patient immediately improved. “Twice more, we tried to stop her treatment.” Each time, her condition deteriorated rapidly. And each time it rebounded as soon as Kinasewitz re-initiated treatment with Xigris. Eventually, the patient recovered. But Kinasewiz is convinced “she wouldn’t have without the drug.”
Dr. Alison Fox-Robichaud, a physician-researcher at McMaster University in Ontario who chairs the examination committee for critical care for Royal College of Physicians and Surgeons of Canada, also participated in the clinical trials and continued to administer Xigris afterward. “I gave it to patients in whom I’m absolutely certain it made a difference in their immediate outcomes: young people at death’s door, a gentleman who was dying on multiple medications,” says Fox-Robichaud. But she’s quick to clarify that Xigris was no magic bullet. “I’ve had at least two serious bleeding problems, so it’s not a drug without risk.” Still, she says, “For the people where nothing else that you are doing is working, that is the one thing I could say turned the corner for them.”
One Last Hope
After his father left the hospital to get him some clothes and reading materials, Ryan Eisner began to shake uncontrollably. He recalls someone telling him he needed a breathing tube inserted to save his life. “You have to agree,” the person told him.
“Yeah,” Ryan responded. “Okay.”
Then it all went black.
The infection, which had apparently started with a respiratory virus and blossomed into pneumonia, had now leaked from his lungs into his bloodstream. In response, his immune system had activated its fail-safe mode, launching every white blood cell in a last-ditch effort that destroyed friend and foe alike. Ryan’s body was in septic shock, and it was literally killing itself.
Doctors sedated him and put him on a respirator. But his condition failed to stabilize. Every hour brought a new problem, and soon his heart began to give out. Then his lungs. Family and friends had gathered in the waiting room, keeping a vigil, hoping for good news. But there was none. Finally, the doctors told the Eisners there was little they could do for Ryan.
Nine years later, the memory still haunts Karen.“All the tubes coming out of him. Catheters here and there.” She goes quiet. ““You can’t imagine how hard it is to see your child like that.”
Ryan, though, still had one thing going for him. Despite the fact that all of his other organs were shutting down, his kidneys continued to function, keeping his blood composition stable and preventing his body from shutting down completely.
There’s a final Hail Mary we can try, his doctors said. It’s a drug that may not work, and it has the risk of causing potentially fatal bleeding.
“They told us, ‘It’s the only thing we can do to try to keep him alive,’” remembers Karen. Her husband’s cousin, a doctor who’d been advising them, encouraged them to try the drug. “He said, ‘It really is your only choice.’”
The hospital didn’t even have the drug on hand, so it had to be flown in. Then the doctors injected Xigris into Ryan’s I.V. line and waited.
Waking From a Nightmare
Ryan remembers three dreams from that time of unconsciousness. In the first, he could see his parents in their home, a bright light bathing them. But they were far away, and he couldn’t reach them. He was trapped in a dark place, with dirt pouring over his body.
He found himself in some sort of athletic facility in the second dream. That felt sort of familiar, like basketball practice. Except he felt like he was someone else. Everybody around him wore headphones that provided them with some sort of vital fluid. But he had no headphones; he also received no sustenance.
The third dream began with Ryan rising from a tub of water. As he gulped down air, he realized that an Indian doctor sat next to him. “It’s time to go home,” the man said. And what seemed like an instant later, Ryan awoke in the hospital room.
He saw his mother first. And there was his father. Oh, and he noticed a bird perched on his foot. No, he knew that wasn’t really there; it must be the narcotics they’d given him. But that catheter running from his neck to his heart? That was real. And so was the tube in his mouth.
After the doctors removed the tube, someone asked him what day it was.
Ryan’s mind felt clouded, slow, but he tried to do some calculations. He’d first gotten sick on Tuesday, come to the hospital Thursday. A few days had probably passed since. “Monday?” he guessed.
It was Friday. He’d been in a medically induced coma for eight days.
Sepsis had devastated Ryan’s body. He’d lost 30 pounds. For days, he couldn’t lie down for fear that fluid would pool in his lungs and prevent him from breathing. Doctors gave him three blood transfusions a day, and his fever persisted. His white blood count was nowhere close to normal. And his legs were so weak that he could no longer walk. “I wasn’t out of the woods by any stretch of the imagination,” he says.
Over time, though, he improved steadily. His fever broke, and he began to add some of the weight he’d lost. He relearned how to walk. “He was so fragile,” says Karen. “He was in pain. He was scared.” She slept next to her son in his hospital bed each night, worrying over everything. “I felt like I had to save his life the whole time.”
Three weeks after he’d first been admitted to the hospital, Ryan was discharged. He returned to school full-time in the spring semester, taking classes and working himself back into shape. The next year, he rejoined the basketball team. By the end of the season, he’d moved from the bench back into the starting lineup, scoring in double digits in 7 of his final 10 games. A few months later, he graduated with his economics degree.
“He’s had some tough luck,” says Mitchell. “In high school, he was on a Division I course until he tore his ACL. Then he got about as sick as a human can get, and I never thought he’d do anything again. But after the sepsis he said, ‘I’m not going to sit there and sulk. If it didn’t kill me, it made me stronger.’ He’s a very resilient kid.”
Today, Ryan works as an account executive for a commercial moving company in Queens. He lives in Manhattan and still plays competitive basketball in a men’s league. Following his illness, he went to doctors frequently. Each time, he feared they’d tell him they’d found something terrible, some hidden consequence of his bout with sepsis that only now was rearing its ugly head. But the doctors didn’t. They told him he was fine. Still, even seven years later, his parents worry whenever he sniffles or coughs. And, admits Ryan, “There’s not a day that I don’t think about it.”
He’s started volunteering for the Sepsis Alliance, using his own experience to help raise awareness. Maybe, he thinks, if more people knew about the deadly illness, more lives could be saved.
“He’s emphatic about helping people learn about this condition,” says Mitchell. “If he can save somebody’s life, he’d be the first guy to do it.”
As for his own life, Ryan can’t say what, exactly, rescued him from death. After all, he was in a coma at the time. But, he says, “I’m under the impression that Xigris was the miracle drug that helped me.”
Karen Eisner, though, harbors no doubts. “I know that drug saved his life. Thank God for Xigris.”
The End for Xigris
While the story of Ryan Eisner has a happy ending, the story of Xigris does not.
In the face of ongoing concerns about its effectiveness, Eli Lilly conducted a second clinical trial to assess the drug. But unlike the initial trial, this one showed that patients treated with Xigris fared no better than those who did not receive the drug. When Lilly received the results of the study in 2011, it pulled the Xigris from the market.
OMRF’s Dr. Charles Esmon had spent years of his life doing the pioneering research that led to the creation of Xigris. When he learned that it would no longer be available to treat critically ill patients, he thought “it was very unfortunate.” But Dr. Naomi Esmon, his wife and life-long research collaborator, had a more visceral reaction. “I cried. Out of frustration and sadness. And I thought, ‘People will die without this drug.’”
Indeed, through the years, the Esmons had read about cases like Ryan’s. And they’d met people who felt certain that Xigris had saved them or a family member. From these accounts, the Esmons developed a theory: While the drug may not have worked in everyone suffering from severe sepsis, for particular groups of patients it could mean the difference between life and death.
Charles Esmon hypothesizes that one group consists of people who, like Ryan, were young and healthy prior to developing sepsis. “In the clinic, many of the patients treated for sepsis will also have hypertension, atherosclerosis, diabetes. All of these co-morbidities create complications.” So he’s not surprised that Xigris didn’t prove effective in every case. “A one-size-fits-all approach was probably not feasible.”
The University of Oklahoma’s Dr. Gary Kinasewitz agrees. “I still think there are patients who would benefit from Xigris,” he says. Like Esmon, he believes that young, previously healthy patients would be one such category, but he also cites sepsis cases stemming from a rare form of infection as another example. But, he says, “When you have a clinical trial, you have very broad criteria.” So only a small portion might respond to Xigris. And in a clinical trial involving thousands of patients, those cases would be no more evident than needles in a haystack.
Another complicating factor, says Kinasewitz, is that physicians have improved the level of care for sepsis since Xigris first came on the market in 2001. “Up until the late 1990s, many physicians didn’t recognize sepsis or treat it with urgency,” he says. “Since that time, there’s been an emphasis on early identification and intervention”—with antibiotics to stem the infection, I.V. fluids to maintain blood pressure, respiratory treatment to maintain oxygen levels. The result, he says, is that more patients are surviving. “So it’s harder to show the benefit of any therapy like Xigris,” especially if doctors don’t give it until all other treatments have failed and the patient is nearly dead.
If nothing else, says McMaster University’s Dr. Alison Fox-Robichaud, she would like to have the drug available for situations like Ryan’s. “This was our most desperate measure to try and reverse a patient’s shock when nothing else was working. So what do we do now when we get that case?”
A Bittersweet Legacy
With Xigris gone from the market, critical care physicians no longer have any compounds specifically approved to treat sepsis. Yet against the backdrop of the drug’s failure and the hundreds of millions of dollars Lilly incurred in clinical trials, pharmaceutical companies have shied away from further efforts to develop new therapies for the illness.
In his laboratory at OMRF, Charles Esmon has identified another protein—this one called a histone—that appears to play a crucial role in the body’s inflammatory and coagulation responses. He’s now working on histone-based therapies for traumas like car accidents and gunshot wounds. Down the line, he may also target organ transplant and stroke. Yet even though experimental results indicate that blocking histones might offer a promising new method for treating sepsis, he’s decided not to explore this avenue. Quite simply, he says, it comes down to money. “The costs of pre-clinical and clinical trials are prohibitive without a drug company on board.”
Still, he looks with satisfaction on the work that started at the stockyards all those years ago. “The insights we gained are very fundamental. All that stuff is now in the major textbooks.” He ticks off a list of conditions—cancer, Crohn’s disease, diabetes, thrombosis—where researchers are now studying the role of activated protein C.
But what about sepsis? Was that just a case of shooting at the wrong bullseye?
“It was the most rational target at the time,” he says. “We showed that activated protein C should work against sepsis. And it did work. I’m 100 percent convinced it saved some lives.”
Karen Eisner, for one, would agree.


